Sometimes there is no other way to say it than through humour. We have taken the most vulnerable in society, and we have lied to them. We have lied as a profession. We have allowed our "regulators" to lie and to collude with lying. The best and most intelligent of our profession have remained silent.
This is the classic description of the research method in these trials:
Monty Python: The Gathering Storm - Part II
"Who's gonna investigate the man who investigates the man who investigates me" was the refrain of "The Investigator's Song", words and music by Harold Rome/Zero Mostel in 1947. The song's final line: "One more problem puzzles me; Pardon my strange whim. But who's gonna investigate the man who investigates the man who investigates... him?"
(The People's Song Book, Waldemar Hille, ed., Boni & Gaer, 1948)
Earlier|Later|Main Page
Tuesday, February 26, 2008
Monday, February 25, 2008
Sydney Taurel, Lilly CEO: What's he smoking?
 When faced with an uncertain course of action or a moral dilemma, I generally ask myself "What would the Lone Ranger do (WWTLRD)?"
When faced with an uncertain course of action or a moral dilemma, I generally ask myself "What would the Lone Ranger do (WWTLRD)?" Sydney Taurel, CEO of Lilly has just announced that he has Benjamin Franklin on his shoulder to act as instigator for his ideas and "role model".
Yes that's the Ben Franklin, innovator, inventor and general good bloke. The Franklin who stressed that the new republic could survive only if the people were "virtuous in the sense of attention to civic duty and rejection of corruption". The Franklin who actually invented stuff, and who "made no effort to patent or profit from any of his inventions" (though Ben would have had no problem with honest profit from innovation). This is the Franklin who believed in free speech and liberty.
"They that can give up essential liberty to obtain a little temporary safety deserve neither liberty nor safety."
-- Benjamin Franklin, Historical Review of Pennsylvania, 1759
"If all printers were determined not to print anything till they were sure it would offend nobody, there would be very little printed."Perhaps Taurel sought advice from Ben before his company bullied academics, lawyers and patients in a foolish attempt to prevent publication of the Zyprexa documents.
-- Benjamin Franklin, 1730
A revised academic analysis of Lilly's decisions needs to take place through this new prism.
- Would Franklin have suppressed data about several deaths in a secret clinical trial that was not published or conveyed to doctors?
- Would Ben have funded such stellar and honorable scientists as Martin Keller and Charles Nemeroff?
- Would Ben have threatened legal action against the British Medical Journal on semantic grounds to do with the meaning of the word "missing" while ignoring the real issue ("BMJ is standing by its more important claims that Lilly was aware of some of the drugs adverse effects as early as the 1980's, yet tried to minimise their likely negative effects on prescribing")?
- Would Franklin, the innovator, have attempted to maintain monopoly sales of his third rate antipsychotic drug (Zyprexa) after his patent ran out - through use of a trick? Seemingly Lilly persuaded someone to grant an extra patent on the irrelevant basis of an amateurish study in a few dogs which suggested olanzapine might be good for your cholesterol! Perhaps the patent prevented Lilly from properly conveying to doctors and patients the full extent of drug-induced diabetes and early death. That sure sounds like Franklin to me.
- Would Franklin have done this, or this, or this, or this, or this?
See here for some more on Sydney Franklin Taurel's comments in his "Franklin" speech.
Earlier|Later|Main Page
Sunday, February 24, 2008
BMJ Advertising Watch : 23 February 2008 - More smoke
 This is the British Medical Journal Advertising analysis for this week.
This is the British Medical Journal Advertising analysis for this week.This issue includes an article by Andrew Jack of the Financial Times on the crisis of "Big Pharma" (BMJ 336:418-9 "Balancing Big Pharma's books). The article completely misses the point. If the point is missed there is no chance of solving the crisis. The real long-term problems facing "Big Pharma" (a science based industry) are not difficult to understand. They are:
- Multiple instances of overt scientific fraud
- Regulatory collusion with that fraud
- Attempts to cover-up that fraud and to redefine the meaning of science itself
- Provision of misinformation and malinformation to doctors and patients
- Government and regulatory collusion to subvert the free market and to prevent consumer litigation
- Refusal to allow science to be properly scrutinized
- Increasing evidence that the peer reviewed scientific literature cannot be trusted
- Internal incompetence and a lack of scientific interchange that prevents picking of even low-hanging fruit. Midgets cannot reach that high, especially when all the giants have been removed.
"It reflects public opinion that is risk averse, sparked by fears such as the reported patient deaths caused by merck's painkiller Vioxx, or GSK's diabetes drug Avandia. Cautious regulators have responded by imposing ever tougher barriers that must be overcome to approve new medicines."Anyone who wishes this industry well (as I do) must realize that to summarize the problem as a public relations issue is not going to help anyone - least of all the industry itself. The health of this industry (including its long-term financial health) would benefit if a few of its leaders were sent to prison.
There was however a decent article by Ray Moynihan on the subversion of Medical Education by commercial companies. The "Better Together" advertisement for Ezetimibe did not appear this week. Neither did the problematical testosterone advertisement.
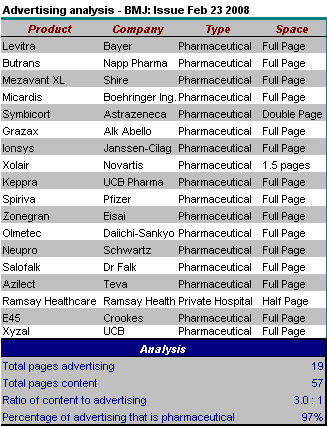
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are advertisements for the BMA, products of the BMJ/BMA/BNF or the government.
The BMJ continues to advertise itself to advertisers thusly:
"We protect our reputation by careful balance of editorial and advertising, which means your messages will always stand out".Here is an accumulated analysis
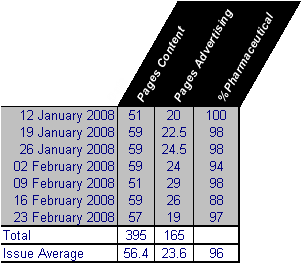
Click here for collated BMJ Advertising analyses.
Earlier|Later|Main Page
Wednesday, February 20, 2008
ENHANCE trial - mystery solved: CEO sees outcome in piece of toast
 PRESS RELEASE
PRESS RELEASESchering Plough CEO Sees Image of ENHANCE Trial Outcome in Piece of Toast
For Immediate Release: 20 February 2008
Amazing Toast provides explanation
(PMPA-London) There has been much excitement over the mysterious prediction of the Vytorin clinical trial (Enhance) and how and what Schering Plough knew and when. Schering Plough has been dogged by accusations and questions about predictive sales of stock, reporting delays and misconduct. There have been questions about mathematical expertise and honesty. Now it appears that the mystery is solved.
An unnamed insider initially reported that a Schering Plough executive was about to eat his breakfast, when an unusual toast pattern caught his eye. "I was about to butter my toast when I realized that there was an unusual pattern of darker crumbs which meant that the Enhance trial was a bust". "It was the beginning of the end, and I immediately went out and sold £25,000,000 worth of my company stock" the executive added.
The actual piece of toast has been retained by Congressional and State investigators and the original toast is copyright to Schering-Plough CEO Fred Hassan. We can therefore only show this image of an unmanipulated slice of toast.
Ever since news of the parallel scientific universe of the ENHANCE study made headlines, Schering Plough and Merck have been inundated with requests to explain several mysterious events. "Now we are satisfied that everything is fully explained" said Hassan. "There has been no fraud. We need to look at the totality of the evidence, including the toast."
"This is astounding news" said Dr Nissen, "seeing is not believing".
"God in heaven forbid that a company profit from helping sick people" said a spokesperson from the Center for Medicine in the Public Interest (Drug Wonks). "Why don't we just not offer any treatment and then we will never have to worry about being accused of conducting shoddy science". "We'll just have thousands of people dying of heart attacks all over the place. Of course there will be arguments about the meaning of the toast. It remains a pity, though, that so much premature confusion has been created in the minds of the public simply by individuals who want science to work in the way it has traditionally worked".
If you'd like more information about this topic, or to schedule an interview with Fred Hassan, please call Carrie Cox at 666/25-MILLION or E-mail Carrie at carriecox@transparency.com
50% of readers found this article helpful.
Earlier|Later|Main Page
Sunday, February 17, 2008
BMJ Advertising Watch : 16 February 2008 (All hail, Delusion)
All hail, Delusion! Were it not for thee
The world turned topsy-turvy we should see;
(Mumfrey Mappel)
This is the British Medical Journal Advertising analysis for this week. The BMJ continues to advertise itself to advertisers thusly: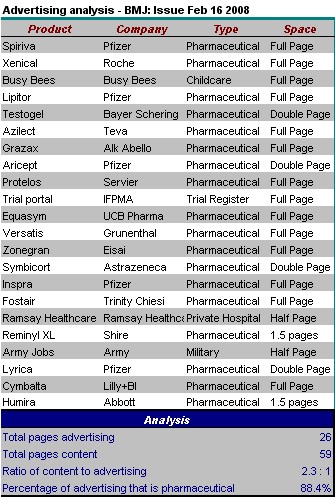
Comment: A full three pages of advertising was devoted to something other than Pharmaceuticals (11.6% of total). The 11.6% comprises an advertisement for the army, half a page on Ramsay Healthcare (a private hospital network with links to the Labour Government), a clinical trials register, and child care provision. There is nothing at all in the BMJ about ongoing developments in the scandal of Ketek. There is not a word about the further findings of manipulated results in Seroxat/Paxil clinical trials. UK doctors seemingly have no interest in the recent revised estimates of the number of individuals who are likely to have died (22,000) as a result of the failure by Bayer to disclose trasylol data in September 2006. There is still nothing of any substance on the Ezetimibe scandal. The "Better Together" advertisement for Ezetimibe did not appear this week. The testosterone advertisement continues to appear.
Click here for collated BMJ Advertising analyses.
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are advertisements for the BMA, products of the BMJ/BMA/BNF or the government.
Earlier|Later|Main Page
The world turned topsy-turvy we should see;
(Mumfrey Mappel)
This is the British Medical Journal Advertising analysis for this week. The BMJ continues to advertise itself to advertisers thusly:
"We protect our reputation by careful balance of editorial and advertising, which means your messages will always stand out".
Comment: A full three pages of advertising was devoted to something other than Pharmaceuticals (11.6% of total). The 11.6% comprises an advertisement for the army, half a page on Ramsay Healthcare (a private hospital network with links to the Labour Government), a clinical trials register, and child care provision. There is nothing at all in the BMJ about ongoing developments in the scandal of Ketek. There is not a word about the further findings of manipulated results in Seroxat/Paxil clinical trials. UK doctors seemingly have no interest in the recent revised estimates of the number of individuals who are likely to have died (22,000) as a result of the failure by Bayer to disclose trasylol data in September 2006. There is still nothing of any substance on the Ezetimibe scandal. The "Better Together" advertisement for Ezetimibe did not appear this week. The testosterone advertisement continues to appear.
Click here for collated BMJ Advertising analyses.
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are advertisements for the BMA, products of the BMJ/BMA/BNF or the government.
Earlier|Later|Main Page
Thursday, February 14, 2008
What is the half-life of a pharmaceutical scientific scandal?
Using Google Trends it is possible to plot the frequency of google searches against time, as well as the incidence of news reports for particular key words (with flags showing the timing of key incidents). I thought it would be interesting to look at a few scientific scandals![[half life scientific scandals]](http://www.thejabberwock.org/blog/2/halflife.gif)
The half-life is about 3 weeks, and is fairly reproducible. Patient deaths and other accumulative effects are not shown.
Earlier|Later|Main Page
- Vioxx
- Vytorin, Zetia
- Avandia
The half-life is about 3 weeks, and is fairly reproducible. Patient deaths and other accumulative effects are not shown.
Earlier|Later|Main Page
Wednesday, February 13, 2008
Jean-Pierre Garnier of GSK calls for a "sophisticated" scientific debate
 Apparently journalists and scientists are responsible for unsophisticated discussion of scientific misconduct involving GlaxoSmithKline products (Avandia, Seroxat/Paxil). So says Jean-Pierre Garnier chief executive of GlaxoSmithKline.
Apparently journalists and scientists are responsible for unsophisticated discussion of scientific misconduct involving GlaxoSmithKline products (Avandia, Seroxat/Paxil). So says Jean-Pierre Garnier chief executive of GlaxoSmithKline. "My wish for the media is to be more sophisticated when they report scientific news," he said at the presentation in London. "Debates now are being thrown into the public domain before scientists have given their opinion."Read on (Glaxo chief curses media and issues profit warning).
I am a scientist and a doctor Mr Garnier ....... and the science stinks. That's my opinion. How does one have a "sophisticated" discussion about scientific misconduct?
They just can't stop themselves - first looking to discredit scientists, then to discredit patients, then to discredit journalists - instead of addressing the shortcomings of their science and ethics.
Never mind the non-transparent science. Never mind the apparent cheating of results in Paxil clinical trials. Never mind the selective publication of "positive" data. Never mind the false and evidence-free statements made about the safety of Paxil. Never mind the bullying of academics, witholding of information from prescribers, threats of legal action, involvement with the UK government, and non-existent criminal self investigations. Never mind Keller, Buse, Laden or study 329. Never mind the patients. Never mind the failure to answer actual scientific questions.
To quote Matthew Holford:
He's got a f_cking nerve to demand that "scientists" (all scientists, or just the ones that agree with and are paid by GSK) are the only ones who are able to proclaim blatantly evident truths. We have only to read the correspondence between McCafferty, Oakes, Keller and Laden (who were responsible for the travesty of science that was the write-up of Paxil Protocol 329).
Quite
Your company disobeyed the rules of science Jean-Pierre Garnier.
The scientific debate cannot be "sophisticated" because there is no real science.
Sales are plummeting and the stock market isn't too pleased. That is excellent in my view. It is about time the stock market started realizing that in a "science based" business, what matters is the quality, transparency and honesty of the science, not the quality of the spin, cover-up and regulatory collusion. It's called the free market. Thinking patients are starting to take notice too.
And what useless journalism in this Guardian piece.
Earlier|Later|Main Page
Tuesday, February 12, 2008
Micro Statistics Tutorial 07: Lessons from honey bees
Here is some correspondence in Science 30 years ago in response to a graph and statistics in a paper by Roubik (Science 1978: 201;1030).


Which prompted Robert Hazen to respond (Science 1978 202:823):


I liked Hazen's response and the subsequent response by Roubik (not shown here). At least this is proper science.
When things are visible and transparent they can be discussed. Despite the obvious over-fitting of data, the Roubik's paper was open and transparent (unlike a lot of the pharmaceutical literature). At least the data were shown.
Misleading graphs formed part of the attempt by Procter and Gamble Pharmaceuticals (P&G) to interfere with scientific evidence about their osteoporosis drug Actonel. The problem was that it was not possible for anyone to know this (including the authors and scientists involved) because there was no data. This was compounded by further spinning of words in the embarrassing admission of guilt over the first of the three manuscripts. Watch this space.
Scientists may disagree about the presentation of data, but there can be no legitimate debate when that data is not available, even to the authors.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Which prompted Robert Hazen to respond (Science 1978 202:823):
I liked Hazen's response and the subsequent response by Roubik (not shown here). At least this is proper science.
When things are visible and transparent they can be discussed. Despite the obvious over-fitting of data, the Roubik's paper was open and transparent (unlike a lot of the pharmaceutical literature). At least the data were shown.
Misleading graphs formed part of the attempt by Procter and Gamble Pharmaceuticals (P&G) to interfere with scientific evidence about their osteoporosis drug Actonel. The problem was that it was not possible for anyone to know this (including the authors and scientists involved) because there was no data. This was compounded by further spinning of words in the embarrassing admission of guilt over the first of the three manuscripts. Watch this space.
Scientists may disagree about the presentation of data, but there can be no legitimate debate when that data is not available, even to the authors.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Sunday, February 10, 2008
Vytorin - the mechanism for no-clinical-benefit ?
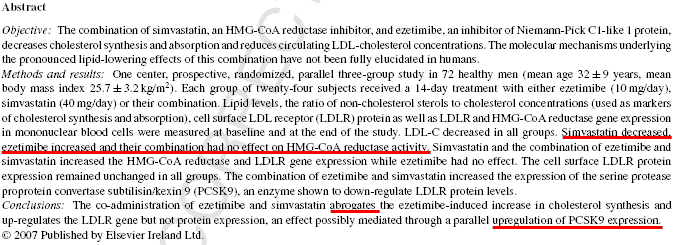
This pre-print manuscript (in press, Atherosclerosis) doesn't seem to have been mentioned on a single blog - so I thought I would stick it up here. Could it explain all sorts of anti-pleotropic effects, and possible paradoxical worsening of atherosclerosis (or lack of effect) of Vytorin in the ENHANCE study?
Any lipidologists out there please interpret.
Ioanna Gouni-Berthold et. al. Atherosclerosis (2008) in Press: Effects of ezetimibe and/or simvastatin on LDL receptor protein expression and on LDL receptor and HMG-CoA reductase gene expression: A randomized trial in healthy men.
Earlier|Later|Main Page
Any lipidologists out there please interpret.
Ioanna Gouni-Berthold et. al. Atherosclerosis (2008) in Press: Effects of ezetimibe and/or simvastatin on LDL receptor protein expression and on LDL receptor and HMG-CoA reductase gene expression: A randomized trial in healthy men.
Earlier|Later|Main Page
Micro Statistics Tutorial 06: Histograms - The Vytorin data so far
Drawing histograms is a useful skill. Choosing the correct number of bars (size of interval) is important. Too few yield an uninformative plot. Too many will be difficult to read. This shows the number of studies designed to prove any clinical benefit of the drug Vytorin (zetia ezetimibe/simvastatin-combination) and the outcome.
Figure 1: The data so far
On a serious note: It is always important to visualize data before doing complicated statistical tests.
PLOT THE BLOODY DATA. That is the most important rule of statistics (and of honest reporting of findings).
To draw a histogram for continuous data, you need to group measurement into discrete intervals. There is some "best" number of intervals that maximizes visual information. Several scientific papers have been written on the optimum number of intervals (K) given the number of data points (N). The Sturgis formula (1) states:
K = 1 + 3.322 log10(N)
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Figure 1: The data so far
On a serious note: It is always important to visualize data before doing complicated statistical tests.
PLOT THE BLOODY DATA. That is the most important rule of statistics (and of honest reporting of findings).
To draw a histogram for continuous data, you need to group measurement into discrete intervals. There is some "best" number of intervals that maximizes visual information. Several scientific papers have been written on the optimum number of intervals (K) given the number of data points (N). The Sturgis formula (1) states:
K = 1 + 3.322 log10(N)
- Sturgis, H.A., “The Choice of a Class Interval”, Journal of the American Statistical Association, Vol. 21, pp.65-66, March, 1926.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
BMJ Advertising Watch : 09 February 2008 (a difficult balance)
Balancing the truth is a difficult task for a scientific journal. This is the British Medical Journal Advertising analysis for this week. The BMJ advertises itself to advertisers thusly:
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are advertisements for the BMA, products of the BMJ/BMA/BNF or the government.
![[BMJ Ad Watch]](http://www.thejabberwock.org/blog/2/bmj20080209.png)
Comment:
Earlier|Later|Main Page
"We protect our reputation by careful balance of editorial and advertising, which means your messages will always stand out".
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are advertisements for the BMA, products of the BMJ/BMA/BNF or the government.
Comment:
- The BMJ broke all records this week with a stunning balance of 29 pages of advertising (1.7 pages of content to balance each 1.0 pages of pharmaceutical advertising). The proportion of advertising devoted to pharmaceuticals was 98.3%. The other 1.7% was a half page advertisement for Ramsay Healthcare - a private hospital network with links to the Labour Government.
- Discussion about the Ezetimibe scandal: Still -- nothing of any substance. At least the "Better Together" advertisement for Ezetimibe did not appear this week.
- The double page testosterone advertisement (see last week) appears again. Still no mention in the advertisement of the actual science - which shows that testosterone supplementation does nothing much to anything. I wonder whether the BMJ expects that readers will believe the "messages" in their "scientific" pages or the "messages" in their "scientific" advertisements? Wonderful word that -- "messages".
Earlier|Later|Main Page
Saturday, February 09, 2008
Micro Statistics Tutorial 05: Functional Unblinding and Vytorin (Method 1)
As discussed in the last post, concerns have been raised about possible "functional unblinding" in the ENHANCE trial of the drug Vytorin (zetia ezetimibe/simvastatin-combination). In other words "could Schering Plough have cheated by trying to work out the outcome of ENHANCE before the "opening" the unblinding codes".
This tutorial does not address whether they "did it" but evaluates one proposed mechanism for "functional unblinding".
One mechanism is to examine the primary outcome variable for bimodality (two camel-like humps indicating separation of treatment arms). Is this possible? Some bloggers and imaging experts suggest that this might have happened in ENHANCE (See Brandweek, Pharmagossip).
Jack Friday explains the potential mechanism thus:
is this possible?
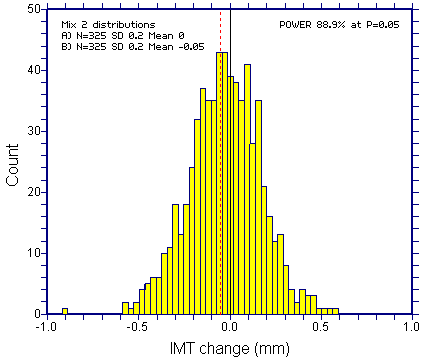
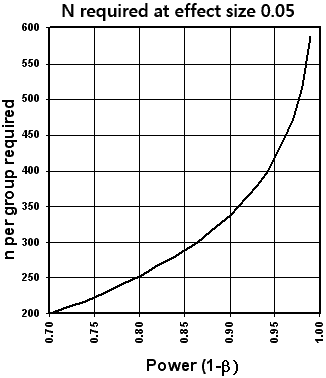
The short answer is no, at least for the primary response variable in a usual clinical trial. It all depends on study power. Usually, trials are sized so as to provide reasonable power (say 70% to 90%). The greater the power, the greater the chance of getting obvious bimodality in unblinded data. However, even at 95% power, bimodality in combined unblinded responses would never be a reliable indicator of a treatment response (or lack of response). It is possible to show this using complicated equations, but a simple graphical example with simulated data (based on the ENHANCE study) is easier.
Enhance had a prior declaration of power as follows:
![[Power statement]](http://www.thejabberwock.org/blog/2/pow1.png)
As discussed in Tutorial 04, this power calculation was slightly wrong. However leave that aside for now.
Assume that the study showed the desired effect of Vytorin. This would mean a "left" shift of 0.05mm (or one quarter of a standard deviation) in the Vytorin arm (with both arms having SD=0.2mm). The plot below shows the distribution of a mix of those two distributions, each at N=325. For convenience, the "placebo" distribution is centered at zero. The vertical dashed line shows the mean of the Vytorin distribution (for an outcome Schering Plough would have deemed as "positive"). This small change that would have been regarded as "positive" is interesting in its own right. Clearly, there is no evidence of bimodality on visual inspection. There are tests for bimodality, but these would not help much more than simple "eyeballing".
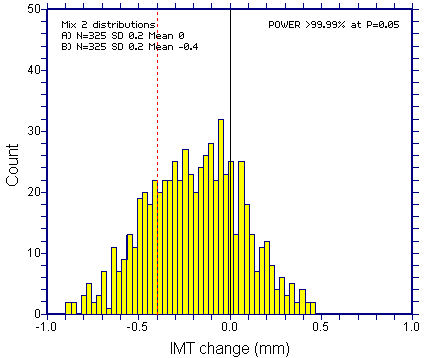
Even if the desired (or expected) treatment effect was eight times bigger at 0.4mm (2 x SD), it would be hard to be sure about bimodality (there would be broadening of the distribution, but this would provide dubious evidence). Such a study would have practically 100% Power (highly unlikely in any study powered on the primary outcome).
Bimodality would however become evident if the SD was halved to 0.1mm in each arm together with the eight fold increase in the treatment effect.
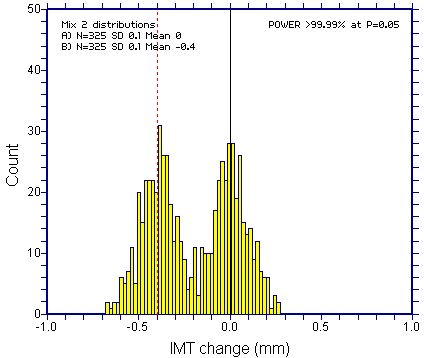
Bottom line: Bimodaility of response (for the primary outcome variable) is not going to be a reliable mechanism to "functionally unblind" a trial.
There are far better methods.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
This tutorial does not address whether they "did it" but evaluates one proposed mechanism for "functional unblinding".
One mechanism is to examine the primary outcome variable for bimodality (two camel-like humps indicating separation of treatment arms). Is this possible? Some bloggers and imaging experts suggest that this might have happened in ENHANCE (See Brandweek, Pharmagossip).
Jack Friday explains the potential mechanism thus:
is this possible?
The short answer is no, at least for the primary response variable in a usual clinical trial. It all depends on study power. Usually, trials are sized so as to provide reasonable power (say 70% to 90%). The greater the power, the greater the chance of getting obvious bimodality in unblinded data. However, even at 95% power, bimodality in combined unblinded responses would never be a reliable indicator of a treatment response (or lack of response). It is possible to show this using complicated equations, but a simple graphical example with simulated data (based on the ENHANCE study) is easier.
Enhance had a prior declaration of power as follows:
As discussed in Tutorial 04, this power calculation was slightly wrong. However leave that aside for now.
Assume that the study showed the desired effect of Vytorin. This would mean a "left" shift of 0.05mm (or one quarter of a standard deviation) in the Vytorin arm (with both arms having SD=0.2mm). The plot below shows the distribution of a mix of those two distributions, each at N=325. For convenience, the "placebo" distribution is centered at zero. The vertical dashed line shows the mean of the Vytorin distribution (for an outcome Schering Plough would have deemed as "positive"). This small change that would have been regarded as "positive" is interesting in its own right. Clearly, there is no evidence of bimodality on visual inspection. There are tests for bimodality, but these would not help much more than simple "eyeballing".
Even if the desired (or expected) treatment effect was eight times bigger at 0.4mm (2 x SD), it would be hard to be sure about bimodality (there would be broadening of the distribution, but this would provide dubious evidence). Such a study would have practically 100% Power (highly unlikely in any study powered on the primary outcome).
Bimodality would however become evident if the SD was halved to 0.1mm in each arm together with the eight fold increase in the treatment effect.
Bottom line: Bimodaility of response (for the primary outcome variable) is not going to be a reliable mechanism to "functionally unblind" a trial.
There are far better methods.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Friday, February 08, 2008
The ongoing story of Wyeth, the FDA and Dr. Hampshire
 This is an ongoing story that should not be forgotten
This is an ongoing story that should not be forgottenFrom the GAP blog:
Last Wednesday, Senator Charles Grassley sent a letter to the HHS Secretary and FDA Commissioner detailing how Wyeth Pharmaceuticals engaged in a smear campaign aimed at discrediting an FDA safety officer (and GAP client) assigned to review one of Wyeth's animal care products. After Wyeth met with FDA officials and presented false and misleading information, the FDA wrongfully removed GAP client Dr. Victoria Hampshire from her position as the drug's reviewer.
Dr. Hampshire previously found that Wyeth's ProHeart 6, a canine heartworm drug, was responsible for contributing to the deaths of hundreds of dogs. After following correct procedures in mid-2005, the drug was removed from the marketplace due to obvious safety concerns.
Grassley's letter details how Wyeth (by its own actions and those of a subsidiary) and the FDA performed several questionable and unethical actions in retaliating against Dr. Hampshire in attempts to get ProHeart 6 back on the market. These include:
- Wyeth's threats to bring down high-level Bush administration pressure on the FDA if they refused to release confidential information.
- Wyeth's hiring of a public relations firm to research Dr. Hampshire's personal property and tax records. This same firm hired consultants to lie and mislead Dr. Hampshire into believing they were veterinarians in a feeble and failed attempt to entrap her into establishing a direct monetary relationship with a Wyeth competitor.
- Wyeth's hiring of a private investigator to 'dig up dirt' on Dr. Hampshire.
- FDA's opening of a criminal investigation into Dr. Hampshire's background, unbeknownst to her. This background saw a Wyeth subsidiary official repeatedly contacting FDA investigators in an attempt to guide their probe.
- FDA's referral of the criminal case, based on Wyeth's misleading "evidence," to the United States Attorney's Office of Maryland. That office declined to prosecute.
The Senator earlier sent a letter to Wyeth, demanding to know whether they paid private investigators to spy on the FDA official. A character called Clint Newsum, Wyeth's counsel, was heavily involved in all this. The same Clint Newsum has been paying off pet owners whose dogs have died after taking Proheart. On this website you can see the letters Clint Newsum has sent to bereaved pet owners, offering them "shut up" money on condition they stop speaking out about ProHeart causing their pet's deaths (and absolving Wyeth of any blame).
Some Wyeth products are:
- Advil
- Advil PM
- Alavert
- Caltrate
- Centrum
- ChapStick
- Dimetapp
- Dristan
- Preparation H
- Robitussin
- Premarin
- Effexor
- Ativan
- Protonix
- Enbrel
- Torisel
- Tygacil
- Zosyn
Wyeth Mission Statement:
At Wyeth, our mission is to bring to the world pharmaceutical and health care products that improve lives and deliver outstanding value to our customers and shareholders.
Earlier|Later|Main Page
Micro Statistics Tutorial 04: Power - Can Schering Plough count?
 As discussed earlier, there have been concerns raised about the possibility of "functional unblinding" in the ENHANCE trial of the drug Vytorin (ezetimibe/simvastatin-combination).
As discussed earlier, there have been concerns raised about the possibility of "functional unblinding" in the ENHANCE trial of the drug Vytorin (ezetimibe/simvastatin-combination).As the first part of this exercise, let us take a look at the POWER of the ENHANCE trial. There is something slightly odd here (I think). The question is: Can Schering-Plough count?
Power, for neophytes out there, is the probability of rejecting a false statistical null hypothesis. The goal is to allow you to decide (in advance of an experiment)
- How many people (or things) you need to study to answer your question
- How likely it is that your statistical test will be able to detect an effect of a given size
- The precise question
- The kind of statistical test that will be used
- The size of the sample (bigger = more power)
- The size of the experimental effects you want to detect (bigger effects need a smaller sample)
- The amount of noise in the measurements (measurement error or biological variability)
Although it is possible to perform power calculations taking account of covariates or confounders (such as baseline IMT, center and so on) this is difficult, and no estimated covariate parameters are provided. One therefore has to assume that the power calculations were carried out using conventional methods (a t-test). In the end Schering Plough recruited slightly more patients than their prior power calculation suggested they should recruit as a minimum. However this is not the issue here. They could also claim that this is just a bit of rounding error (see further discussion in comments). This is again irrelevant - the fact remains that it is not possible to add two and two from the numbers they give, or to resuscitate their rather simple calculations. This bypassed the entire system of safeguards that is supposed to check these little details.
So on to the power. Well, as far as my humble brain can establish, Power for N=650 is in fact 88.9%, not 90%.
The required N for 90% Power, 2-tailed alpha 0.05, between group difference of 0.05mm and SD=0.20mm is not N=650.
It is N=674.
A small difference perhaps, but it does tell us something interesting about the process:
- Perhaps I can't count
- Perhaps Schering-Plough or Merck can't count
- Perhaps the authors of the protocol paper didn't read their paper
- Perhaps peer reviewers didn't back-check anything
- Perhaps there is something Merck or Schering-Plough aren't telling
- Perhaps Carrie Smith Cox can only count in units of $28 million
Reference
J. Kastelein, P. Sager, E. de Groot, E. Veltri (2005). Comparison of ezetimibe plus simvastatin versus simvastatin monotherapy on atherosclerosis progression in familial hypercholesterolemia. Design and rationale of the Ezetimibe and Simvastatin in Hypercholesterolemia Enhances Atherosclerosis Regression (ENHANCE) trial. Am Heart J. 2005 Feb;149(2):234-9.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Thursday, February 07, 2008
Micro Statistics Tutorial 03: Asking the right question
 "Cheer up! Have you no aim in life?"
"Cheer up! Have you no aim in life?"She tenderly inquired.
"An aim? Well, no, I haven't, wife;
The fact is -- I have fired." (GJ)
Dave discussed the elements of good statistics in Tutorial 01:
- A decent, honest, well described set of data
- Proper definition of terms, specified in advance
- A clear, well framed and unambiguous question (or problem), specified in advance
- A plan for examining those data, specified in advance
- Honest intent
"If they can get you asking the wrong questions, they don't have to worry about the answers."Here are some others:
(Pynchon T, 1995 Gravity's Rainbow. ISBN 140188592)
It isn't that they can't see the solution.
It is that they can't see the problem.
G.K. Chesterton
First things first, but not necessarily in that order.It is a poor scientist who refuses to explain what question they are answering.
Doctor Who
Example: 1463 days to nothing - The MHRA and the GlaxoSmithKline Criminal Self Investigation
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Wednesday, February 06, 2008
Micro Statistics Tutorial 02: Double Blind (Trust)
Blinding in clinical trials refers to a type of study design. The graphic explains the concept. It does not refer to the hiding of science from authors of papers, "regulators", doctors, or the public.

In a blind study, the researcher or the participant or both (double blind) are blind to (unaware of) the type of treatment being administered. Double-blind trials are more likely to produce objective findings. This is because the expectations of researcher and participant cannot alter the outcome. It also makes cheating more difficult. Practitioners of "complementary" medicine such as bone throwing are not too keen on blinded trials (bone throwing is not yet available on the NHS - but watch this space).
For a good example of blinding in practice see: Vioxx and a quacking duck
A few of us have been agonizing over the potential problem of "functional unblinding" in Vytorin/Zetia trials. This is where effective unblinding happens without officially opening the book of randomization codes. There are a few possible mechanisms for this including a) inspection of treatment surrogates or confounders, b) looking at data distributions, c) inspection of treatment side effects, or d) taking a sneak peek at the codes when no-one is looking. Each of these will form the subject of a later tutorial.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
In a blind study, the researcher or the participant or both (double blind) are blind to (unaware of) the type of treatment being administered. Double-blind trials are more likely to produce objective findings. This is because the expectations of researcher and participant cannot alter the outcome. It also makes cheating more difficult. Practitioners of "complementary" medicine such as bone throwing are not too keen on blinded trials (bone throwing is not yet available on the NHS - but watch this space).
For a good example of blinding in practice see: Vioxx and a quacking duck
A few of us have been agonizing over the potential problem of "functional unblinding" in Vytorin/Zetia trials. This is where effective unblinding happens without officially opening the book of randomization codes. There are a few possible mechanisms for this including a) inspection of treatment surrogates or confounders, b) looking at data distributions, c) inspection of treatment side effects, or d) taking a sneak peek at the codes when no-one is looking. Each of these will form the subject of a later tutorial.
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Micro Statistics Tutorial 01: Lessons from Dave, the forecasting pig
 Most (not all) statistics is about prediction. Forecasting is about prediction of future events (usually, but not always, in advance of those events). For example, Carrie Smith Cox, President of Schering-Plough, dumped $28 million worth of stock before anyone knew about negative studies, altered endpoints or anything at all about the drug Vytorin (ezetimibe/simvastatin-combination). That is an example of forecasting. We might however want to predict events in one group of people, knowing what happened in another group.
Most (not all) statistics is about prediction. Forecasting is about prediction of future events (usually, but not always, in advance of those events). For example, Carrie Smith Cox, President of Schering-Plough, dumped $28 million worth of stock before anyone knew about negative studies, altered endpoints or anything at all about the drug Vytorin (ezetimibe/simvastatin-combination). That is an example of forecasting. We might however want to predict events in one group of people, knowing what happened in another group. Here is where we introduce Dave, the Forecasting Pig (Reuters 31 Jan 2008). Dave lives in Ohio. He opines (or oswines) on US economic status, and is a key statistical tool used by the Ohio treasurer's office. Dave decides between a trough of sugar or one of sawdust to gauge the economy's future. Sadly, better methodologies are available (ask Carrie Smith Cox).
Tutorial take home message:
The ingredients of good statistics:
- A decent, honest, well described set of data
- Proper definition of terms, specified in advance
- A clear, well framed and unambiguous question (or problem), specified in advance
- A plan for examining those data, specified in advance
- Honest intent
Have you had the measles?
If so, how many?
(Armstrong Ward)
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Micro Statistics Tutorials: Introduction
 Some say I should run a series of real-world statistics "tutorials". A bit like the good book Statistics at Square one but in juicier chunks.
Some say I should run a series of real-world statistics "tutorials". A bit like the good book Statistics at Square one but in juicier chunks. The stimulus was the wonderful letter in the BMJ (signed by around 20 statisticians) asserting that EU regulators should employ more card carrying statisticians to "explore methods and data in real depth".
The claim for God-given magical powers of statisticians would carry more credibility if any of the signatories were commentators on instances of blatant fraud in clinical trials, or on the absence of actual data to "explore".
 I like statisticians but they have no such magical powers. Most statistics is (and should be) transparent and straightforward.
I like statisticians but they have no such magical powers. Most statistics is (and should be) transparent and straightforward.Some actual statisticians have screwed up, lied, colluded with fraud, colluded with ghosts, completely misunderstood the science, or agreed to the hiding-away of data. Most have stood by in silence.
Please send along any examples. Here goes - the Scientific Misconduct Blog Micro-Statistics Tutorials. Some will be serious, others couched in frippery.
The usual disclaimer: INAS (I'm Not A [proper card holding] Statistician).
See here for Collated Micro-Statistics Tutorials
Earlier|Later|Main Page
Saturday, February 02, 2008
Updated Political Map of pharmaceutical bloggers
This is the updated "political chart" of pharmaceutical bloggers. For background see here. For details see here. Take the test here.
Clicking individual "dots" should open the respective blogs in a new window. For comparison with historical political figures and UK political parties according to the authors of the test see here.
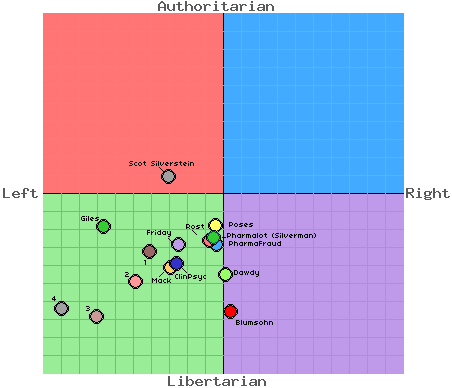
Blogs so far are
Healthcare Renewal (Roy Poses and others) - the serious master of them all
Pharmagossip (Jack Friday) - the less serious master of them all
Pharmalot - and the man behind it - Ed Silverman of The Star-Ledger of New Jersey. Superlative journalism and a key source.
Brandweek NRX and Dr Peter Rost, previous Vice President of Pfizer
Pharma Giles - Good Fun
Pharma Fraud - Doesn't Like J&J particularly
Furious Seasons - Excellent look at seriously bad science in psychiatry
Scientific Misconduct Blog - This blog
Clinical Psychology and Psychiatry: A great blog discussing the malfunction of medical science with an emphasis on psychiatry
Pharma BlogoSphere and much more from John Mack (Editor & Publisher of Pharma Marketing News/Pharma Marketing Blog)
Dr Scot Silverstein, an author at Healthcare Renewal
1, 2 and 3 are three excellent and hard hitting (and deeply depressing) UK-based patient blogs devoted specifically to exposing misconduct and misrepresentation in clinical trials of Seroxat (Paxil) and various aspects of the integrity of GlaxoSmithKline.
1 = Bob Fiddaman Blog
2 = Seroxat Secrets
3 = It's quite an experience: Matt Holford (a compliance lawyer)
4 is Honest Medicine. Julia Schopick created Honest Medicine in honor of her late husband, Tim Fisher, as a way to "work with others to make significant changes to the way people think about, and interact with, our flawed medical system."
This test is significantly flawed, but we'll leave that for another day.
Earlier|Later|Main Page
Clicking individual "dots" should open the respective blogs in a new window. For comparison with historical political figures and UK political parties according to the authors of the test see here.
Blogs so far are
Healthcare Renewal (Roy Poses and others) - the serious master of them all
Pharmagossip (Jack Friday) - the less serious master of them all
Pharmalot - and the man behind it - Ed Silverman of The Star-Ledger of New Jersey. Superlative journalism and a key source.
Brandweek NRX and Dr Peter Rost, previous Vice President of Pfizer
Pharma Giles - Good Fun
Pharma Fraud - Doesn't Like J&J particularly
Furious Seasons - Excellent look at seriously bad science in psychiatry
Scientific Misconduct Blog - This blog
Clinical Psychology and Psychiatry: A great blog discussing the malfunction of medical science with an emphasis on psychiatry
Pharma BlogoSphere and much more from John Mack (Editor & Publisher of Pharma Marketing News/Pharma Marketing Blog)
Dr Scot Silverstein, an author at Healthcare Renewal
1, 2 and 3 are three excellent and hard hitting (and deeply depressing) UK-based patient blogs devoted specifically to exposing misconduct and misrepresentation in clinical trials of Seroxat (Paxil) and various aspects of the integrity of GlaxoSmithKline.
1 = Bob Fiddaman Blog
2 = Seroxat Secrets
3 = It's quite an experience: Matt Holford (a compliance lawyer)
4 is Honest Medicine. Julia Schopick created Honest Medicine in honor of her late husband, Tim Fisher, as a way to "work with others to make significant changes to the way people think about, and interact with, our flawed medical system."
This test is significantly flawed, but we'll leave that for another day.
Earlier|Later|Main Page
BMJ Advertising Watch : 02 February 2008
This is the British Medical Journal Advertising analysis for this week.
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are pages advertising the BMA or products of the BMJ/BMA/BNF.
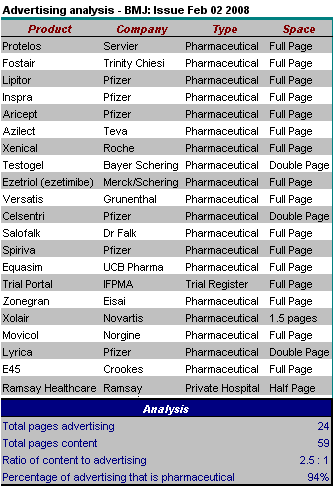
Comment: There were 24.5 pages of advertising (1 page of advertising for each 2.5 pages of content). The proportion of advertising devoted to pharmaceuticals fell to an all time low of 94%. The other 4% was:
There were a few other notable items this issue:
Click here for collated BMJ Advertising analyses.
Earlier|Later|Main Page
Rules: As usual this is for the UK version of the BMJ. The classified advertisement section is excluded, as are pages advertising the BMA or products of the BMJ/BMA/BNF.
Comment: There were 24.5 pages of advertising (1 page of advertising for each 2.5 pages of content). The proportion of advertising devoted to pharmaceuticals fell to an all time low of 94%. The other 4% was:
- a half page advertisement for Ramsay Healthcare (for more about Ramsay and their cozy links with the Labour Government see here)
- a one page advertisement for a register of clinical trials.
There were a few other notable items this issue:
- A letter from a reader (Jeremy Stone) complaining about discordance between a double page advertisement for testosterone supplements in the previous issue, and (on the very next page) a double blind RCT showing that testosterone supplements have no effect on functional mobility, muscle strength, cognitive function, bone mineral density or quality of life. I'll look out for proper referencing in the next appearance of this advertisement. They might even want to reference our paper showing that testosterone supplementation does nothing useful to anything (except plasma testosterone).
- There was a dismal letter signed by around 20 statisticians asserting that the EU regulatory agencies should employ more card carrying statisticians to "explore methods and data in real depth". The plea for employment and the special God-given powers of statisticians would carry more credibility if there were evidence that any of the signatories were regular commentators on instances of blatant fraud in clinical trials (no statistical expertise required) or on the fact that neither regulators nor scientific authors have genuine raw data to "explore" in any case. None (as far as I am aware) have commented on Ezetimibe. Statisticians would also do well to realize that only a few aspects of data integrity are within the special remit of complex statistics. All scientists require raw data.
- There was a detailed Obituary of Moses Judah Folkman (the "father of angiogenesis") by Jeanne Lenzer. In contrast to other Folkman obituaries it did at least mention that he had been forced to "apologise" over scientific fraud (false descriptions of methodology and falsified findings in an NEJM publication).
Click here for collated BMJ Advertising analyses.
Earlier|Later|Main Page
Friday, February 01, 2008
A few notes on the abuse of occupational health procedures
 "Whom the Gods wish to destroy, they first make mad"
"Whom the Gods wish to destroy, they first make mad"-Euripides
Over the past few years I have listened to many cheerless stories of individuals who have exposed unacceptable practices within universities and hospitals. The institutional response is almost formulaic.
A frequent part of the common experience is the abuse of occupational health procedures. Following an incident this week involving a colleague, I have summarised some aspects of UK occupational health law below.
Most of these individuals started with the belief that their institutions would assume responsibility for upholding their own rules of conduct. They assumed that responses would be honest, colleagues and professional bodies would behave honorably, and that someone would take responsibility for the safety of the product (whether that product is a drug, honest science, open academic discourse or care of individual patients).
In reality, most are projected into an Alice in Wonderland world of sham procedures, collusion, lies and bullying. Many become ill (see the case of Dr Z), and some die. Distress signals are used by poor managers to invent "health concerns" and to avoid rational discussion about genuine problems. That hospitals and medical schools abuse their staff through health mechanisms is indicative of deep immorality within these institutions. The process usually starts as an apparent expression of genuine concern about the health of the employee.
Sadly, psychopathic administrators and medical leaders are rarely subjected to psychiatric or medical evaluation.
Employees should almost never agree to an employer's "offer" of health evaluation under these circumstances. When such evaluation takes place, it should only be for the benefit of the employee. Any assertion by the employer that they must have any right of access to health information is illegal and constitutes serious bullying.
Aspects of the relevant law is summarised from these sources: a) Occupational Health Law, 4th Edition, Diana M Kloss ISBN 0632-064978, b) Medical Ethics Today: Its Practice and Philosophy, Veronica English, Gillian Romano-Critchley. 2002 2nd Ed. BMJ Books, ISBN 0727917447
- The physical occupational health (OH) records technically belong to the employer, but the employer has no right of control or access to the information therein.
- OH doctors should have an agreement their employer with regard to confidentiality of records. If the doctor leaves the company, records remain the property of the employer, but should be passed to a new doctor or nurse with the same obligations. If an employee moves to another employment, OH records can only be transferred to the new employer with consent.
- Employers cannot enforce terms in contracts of employment stating that employees must provide copies of medical records.
- OH doctors have a duty of confidence which is the same as that for any other doctor. For example, if an OH physician were to reveal to the human resources department (without permission) that an employee has a drink problem the doctor could be sued for damages. Secretarial staff who have access to confidential information share these obligations.
- According to the General Medical Council there are restricted circumstances under which information could be conveyed by a doctor:
- The patient explicitly consents.
- Some circumstances where the doctor shares information with other health professionals caring for that patient
- Parliament requires disclosure (notifiable diseases, RIDDOR reporting of injuries at work, and more worryingly "terrorism legislation")
- Disclosure may be made to a statutory regulatory body for investigation into a health professional's fitness to practice (it is worrying that the GMC would see fit to incorporate such a provision without detailed qualification)
- Disclosure is in the public interest, e.g. to the police about a serious crime
- If consent is provided, it can later be withdrawn. Consent should be in writing for the protection of the doctor or nurse. Consent should clarify exactly what records may be passed over - not simply "all records". The OH doctor can refuse to accept partial consent if that would be misleading through omission. An OH doctor should not communicate with the patient's own doctor without consent.
- Guidance from the Nursing and Midwifery Council (2002) is more coherent with greater emphasis on the purpose for which information was supplied: "To trust another person with private and personal information about yourself is a significant matter. If a person to whom that information is given is a nurse, midwife or health visitor, the patient or client has a right to believe that this information, given in confidence, will only be used for the purposes for which it was given and will not be released to others without their permission".
- Mere attendance at the OH department does not imply consent.
- Even if an employer is facing legal action by an employee, OH records should not be disclosed to the employer without consent or a court order.
- An occupational health doctor may find that an individual is somehow unfit for a job or that the employee is in danger. This does not justify a breach of confidence. If the danger is to others there may be a case for breach of confidence, but even then this requires very careful deliberation.
- Per the Faculty of Occupational Medicine's Guidance on ethics: "Occasionally the occupational physician ....may find that an individual is unfit for a job where the safety of other workers or the public is concerned. He should then take great care to explain fully why he thinks the disclosure of unfitness is necessary.... Where this is not obtained the occupational physician is faced with an ethical dilemma..... Ultimately, the safety of other workers and the general public must prevail..."
- Occupational health doctors should not become involved in advising employers on the validity or otherwise of sickness absence of an employee. They can however (in consultation with the employee) advise management on potential changes required to the conditions of employment. The doctor may also advise the employer about future employability but without providing clinical details of sickness to the employer.
- Some occupational health records may be of direct relevance to the employer (for example where the employer has a legal requirement to monitor toxic substances). Those records should be maintained separately from other records. Conveying of such records also requires consent.
Earlier|Later|Main Page
Subscribe to:
Posts (Atom)